The following policies and procedures have been established for Mental Health Minnesota’s 988 Lifeline Center. Please refer to this information for direction and clarity on organizational practices. If you have questions, please contact a supervisor or manager.
Confidentiality
All information concerning clients, former clients, donors, employees, volunteers, financial data and business records of Mental Health Minnesota is confidential. All information pertaining to clients (which include any individual(s) seeking information, services, or support provided by Mental Health Minnesota) shall be held as confidential by organizational employees and volunteers. Confidential information must not be disclosed to unauthorized persons, including competitors, reporters, friends, family, or other employees whose duties do not require use of such information.
“Confidential” means that employees are free to talk about Mental Health Minnesota, the program/services they help provide, their position or their relationship with the organization, but employees are not permitted to disclose the names of individuals served or talk about clients served by the organization in ways that will make their identity known (ex. describing a specific interaction). No information may be released without appropriate authorization except in the case of a lifesaving emergency, to be determined in consultation with a supervisor and/or Manager. This is a basic component of client care and business ethics. The Board of Directors, staff and our clients rely on employees and volunteer staff to conform to this rule of confidentiality.
Mental Health Minnesota expects employees to respect the privacy of clients and to maintain their personal and financial information as confidential. All records dealing with specific clients must be treated as confidential. Employees are also responsible for maintaining the confidentiality of information relating to other employees and volunteers, in addition to clients.
All employees are required to acknowledge and sign an agreement to follow the Confidentiality and Non-Disclosure Policy as a condition of employment. Employees who improperly use or disclose confidential business information or program participant information will be subject to disciplinary action, up to and including termination of employment. This policy is intended to protect employees as well as Mental Health Minnesota because, in extreme cases, violations of this policy also may result in personal liability.
Suicide Safety Assessment, Safety Planning and Intervention
Purpose: The purpose of the Suicide Safety Assessment, Safety Planning and Intervention Policy is to determine suicidal risk while allowing suicidal individuals a chance to defuse and take control of their own situation and develop a safety plan before other intervention services are called in.
A Safety Assessment must be completed for any individual who indicates a risk for suicide. To assist with the assessment, Mental Health Minnesota uses the National Suicide Prevention Lifeline’s prompt questions and Safety Assessment items, which include the Lifeline’s Four Core Principles of Assessment (desire, intent, capability and buffers).
Mental Health Minnesota will use the least restrictive intervention possible, such as active collaboration with the contact to secure their own safety. This may include collaboration with other community crisis and emergency services.
Definitions:
Imminent Risk: An individual would be considered at Imminent Risk if the counselor (in consultation with a supervisor, if available) believes that the individual is likely to seriously harm or kill themselves if no actions are taken.
Active Engagement: Intentional behaviors taken by counselors to effectively build an alliance with a person at risk of suicide toward a mutual agreement on actions necessary to reduce risk of suicide through development of a safety plan or accept medical interventions if the person is in the process of a suicide attempt.
Emergency Service Intervention: Actions taken by counselors that are intended to ensure the safety of individuals at Imminent Risk or in the process of a suicide attempt. Emergency service interventions occur when a counselor (in coordination with a supervisor) acts to provide potentially life-saving services on behalf of the individual because the person with thoughts of suicide is unwilling or unable to initiate actions to secure their safety. Mental Health Minnesota should only provide an emergency service intervention without the at-risk individual’s expressed desire to cooperate if they believe that, without this intervention, the individual is likely to sustain a life-threatening injury.
Caller Risk and Lethality: There are three lethality levels when an individual indicates they has suicidal thoughts: High Lethality (in progress or imminent risk), Moderate Lethality (plan), and Low Lethality (thoughts).
- High Risk/Lethality: When an individual is in the process of suicidal action or when suicidal action will likely occur soon.
- Moderate Risk/Lethality: When an individual has a plan for suicide, but no immediate intentions.
- Low Risk/Lethality: When an individual states that he or she has thoughts of suicide or recently had thoughts of suicide and has no plan to kill themselves.
Procedure:
Counselors will use active listening and active engagement to promote the individual’s collaboration in securing their safety. Counselors will use the least invasive intervention. Involuntary emergency interventions are used as a last resort when the person at risk is unwilling or unable to participate in a safe plan to secure their safety.
1. Establish a relationship with the contact
- Positively reinforce the individual’s decision for making the call.
- Be accepting, warm, supportive, non-judgmental.
- Demonstrate confidence and concern.
- Let the person know you are trained to do this type of work (Communicates to the person with thoughts of suicide that you will be able to render the needed help).
- Without alienating the person, get as much identifying information as possible, including:
- Details about the contact (name, address, gender, age, relationships, names of relatives, if they are in their car, etc.)
- If they are alone
- If they have a weapon
2. Evaluate suicidal thoughts/assess the degree of risk
A Safety Assessment must be completed for all individuals contacting the Lifeline Center service. To assist with the assessment, Mental Health Minnesota uses the National Suicide Prevention Lifeline’s prompt questions and Safety Assessment items, which include the Lifeline’s Four Core Principles of Assessment (desire, intent, capability and buffers). The following questions will be asked, and are imbedded in the organization’s data collection form:
- Have you had any thoughts of suicide in the last few days, including today?
- Have you taken any action to harm yourself today?
If the counselor receives an affirmative answer to either of these questions, the counselor should continue with an assessment utilizing the Lifeline’s Safety Assessment items which address the following core principles:
- Desire (suicidal ideation, hopelessness, psychological pain, perceived burden, feeling trapped, feeling intolerably alone, and self-hate)
- Capability (history of suicide attempts, history of self-harm, dysregulation, available means of killing self/others, current intoxication, exposure to another’s death by suicide, history/current violence toward others, substance abuse, sleep disturbance, increased anxiety, mood change, decreased sleep)
- Intent (plan to kill self/others, preparatory behaviors, and expressed intent to die)
- Buffers (immediate supports, reasons for living, ambivalence, social supports, planning for the future, engagement with the helper, core values/beliefs, and sense of purpose)
The assessment should take place through active listening rather than asking specific questions related to the assessment. This assessment should be used as needed by counselors to explore the individual’s resources and strengths, assess current level of safety, determine the most appropriate help to provide, and help further determine the degree of risk by assessing the lethality and probability of an attempt.
If during the assessment the counselor believes that the individual is at low lethality:
- Continue the call/text/chat by providing support, resources and referrals as needed, while listening for any new references to suicide or self-harm.
If during the assessment the counselor believes that the individual is at moderate to high lethality:
- Continue to engage the individual in the call/text/chat
- Immediately alert the shift supervisor, who can then listen in to the call (or watch the transcript as a text/chat occurs) and provide guidance and intervention or emergency service intervention if needed.
3. Begin crisis intervention and learn more about the person’s situation
- Listen to both words and feelings.
- Encourage the expression of feelings (helps to dissipate the intensity).
- Listen to the individual’s statements about dying and living.
- Help to identify and clarify problems, knowing that the person may be emotional, feel uncertain, may not truly understand what his/her needs are, and perceptions may not reflect reality.
- Support the individual’s experience/feelings.
4. Assess the person’s resources
- Explore resource options, including self, formal, and informal resources.
- Ask about previously successful coping strategies and strengths.
- Ask about a significant other, friends, relatives, or neighbors who might be helpful.
- Find out what is still meaningful to the person (i.e., what has kept him or her alive?) if and/or when the person begins to focus on living and the future, stress the importance of whatever the ‘silver lining’ in their life is.
If you determine, after a thorough risk assessment, that the person is at risk (whether high, moderate, or low) but has de-escalated, follow these steps:
- If possible, mobilize the person’s resources
- Build hope for the future, recovery, connecting to others, and living.
- Empower the individual to work towards securing his/her safety.
- Encourage the involvement of others, including current and/or new professionals.
- Provide information about crisis resources, including mobile crisis response, crisis stabilization services, and crisis residential services.
- Encourage face-to-face contact with someone today/tonight (significant other, family, friends, neighbor).
- Collaborate to build a safety plan with the person at risk using the organization’s 988 safety planning tool as a guide.
If you determine, after a thorough risk assessment, that the person is at risk and has not de-escalated, follow these steps:
- Gather information about the individual, including phone number, current location, whether there are others present, and whether lethal means are present.
- Alert your supervisor and provide information and details regarding the situation
- Collaborate to build a safety plan with the person at risk using the organization’s 988 safety planning tool as a guide.
- If the person with thoughts of suicide is willing and verbalizes permission, the counselor can facilitate a “warm hand-off” to the county crisis service based on information collected about the individual’s location. All counselors are trained in how to provide warm hand-offs as part of their orientation, and can consult with the supervisor as necessary.
- If the chat/text gets disconnected or individual ends the interaction before the safety plan can be confirmed, the counselor should try to reach the contact by phone if available. Up to two attempts can be made within one minute. Do not leave a message and only identify yourself as calling from Mental Health Minnesota to the original caller. If the individual does not answer, the counselor should consult with the supervisor. The supervisor will determine whether rescue or a safety check should be initiated based on information about the interaction from the counselor and review of the chat/text transcript.
If at any time you determine that an attempt is in progress or that the contact is at imminent risk:
- Try to get the person to discard the lethal means.
- Ask for the contact to accept life-preserving services such as mobile crisis, police or sheriff to assess their safety.
- If the caller refuses services, but the counselor believes the contact is at imminent risk or a suicide attempt is in progress, the staff member/volunteer should initiate emergency service intervention by contacting 911 dispatch (contacting the nearest 911 center to the individual’s location).
- If the person with thoughts of suicide has already taken action with the potential to cause lethal self-harm, the counselor and supervisor should immediately initiate emergency service intervention. The top priority is to engage in life-saving services. The 988 program manager should be informed anytime that emergency service intervention is initiated/law enforcement support is requested.
- If emergency service intervention procedures are initiated, the counselor should attempt to contact the person with thoughts of suicide by phone, and should maintain contact (via phone, text or chat) until help arrives.
- Supervisors should initiate emergency service intervention if necessary except in an emergency (i.e. supervisor is unavailable and emergency services must be reached immediately to provide life-saving assistance).
- In the event that counselors believe that emergency service intervention should be initiated, they should relay the following information to the supervisor:
- What time the text/chat came in
- How long the text/chat has been ongoing
- Why you feel the caller needs on-site emergency services (specific actions the individual has taken and at least one suicidal phrase the contact has said)
- Details that identifies the individual such as name, address, gender, approximate age, relationships, names of relatives, type of car, part of the license plate number, etc.
- Any safety concerns that emergency services responders should be aware of (weapons, pets, etc.)
- If anyone else is present
Confirming Emergency Service Contact and Safety of Those with Imminent Risk:
When possible, the counselor will remain on the line with the individual until the emergency service provider has arrived and their presence is apparent to the counselor.
If the counselor is unable to remain on the line or the call/text/chat is disconnected before confirming that emergency services has arrived, the supervisor should contact the 911 dispatch will be contacted to determine whether they were able to locate the person and provide emergency assistance.
Follow-Up for When Emergency Services Contact is Unsuccessful
When emergency service contact was attempted but did not occur, the following procedure is used to determine caller safety:
- Contact the individual at risk to assess their current risk status and continuing need for services/referrals.
- Re-assess the individual for suicide risk using the approved instrument(s).
- If agreed upon and necessary, connect the individual with the appropriate mobile crisis team for follow-up.
- If necessary due to imminent risk of suicide, inform local law enforcement authorities or other appropriate first responders of the situation and requesting continued safety checks until the safety status of the individual at risk can be confirmed.
Collaboration with Emergency Services and Mobile Crisis Response
Mental Health Minnesota will establish and maintain both formal and informal relationships with emergency service providers and mobile crisis response teams to ensure a trusting and collaborative response to suicide risk and attempts. These relationships may include but are not limited to mobile crisis response teams, hospital emergency departments, 911 centers, police/sheriff departments, and EMS/fire departments.
Supervisory Consultation
At least one experienced counselor/supervisor will be designated on each shift as a shift supervisor, and if necessary, an offsite supervisor can be contacted by cell phone. To ensure that emergency service interventions occur only when necessary and appropriate, supervisory consultation should occur before, during and after instances where emergency service intervention has been initiated for callers by Mental Health Minnesota staff.
In the event that a supervisor is not consulted during an emergency service intervention call, they should at least be made aware of the event soon thereafter so they may review it for ongoing training and procedure development purposes. This should evaluate both the process (how was the decision made) and documentation related to the call. Documentation should minimally include risk assessment information (noting the presence of imminent risk) and indicate that less invasive courses of action were either inappropriate for the situation or declined by the caller.
All interventions that have resulted in requesting a PSAP to dispatch an emergency service intervention, either voluntary or involuntary, must undergo a supervisory review. This must occur in a timely manner (ideally within 72 hours) and include both crisis counselor and supervisor involved in the request.
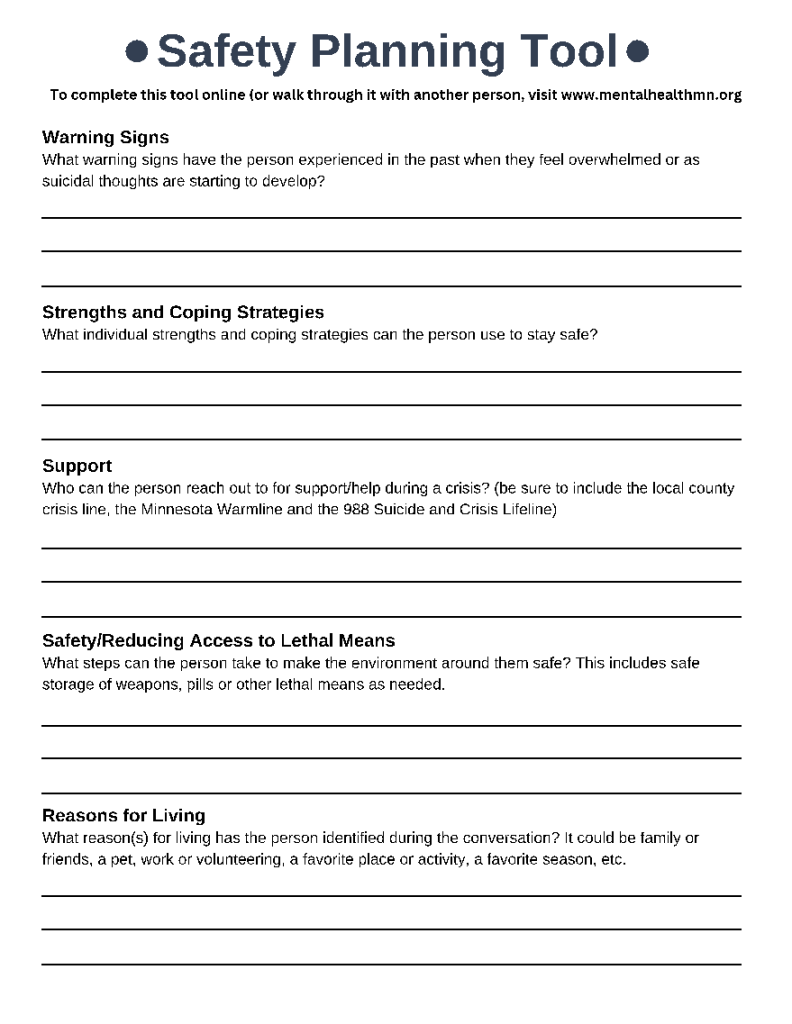
Safety Planning
Purpose: Safety planning is a critical piece of providing service to those reaching out to the 988 Suicide and Crisis Lifeline. Safety planning can help address concerns related to an individual’s immediate safety, including access to lethal means. It can also provide a roadmap for the individual experiencing crisis and/or suicidal ideation to help them connect to support, tools, resources and services.
Safety planning should be a part of any text/chat interaction where the individual indicates that they have experienced suicidal ideation or have a plan for suicide. Safety planning via text and chat requires the counselor to ask open questions of the individual to determine steps that the individual can take to help keep themselves safe. Much of the conversation around safety planning is something that can occur throughout the text/chat interaction.
After working with an individual to develop a safety plan, the counselor should confirm the steps that the individual has indicated they will take to keep themselves safe, and ask the individual to confirm the plan and/or repeat it back to them in their own words. (Ex. Get them to say this back to you in their own words: details we have planned (i.e., “I plan to contact my sister and explain my situation” or “Now that we have informed my spouse, I will disclose where I have stockpiled pills”).
Safety plans should include making the environment safe, getting rid of the means that they plan to use for suicide (i.e. gun and ammunition kept at friend’s house, pills kept in a lockbox, with trusted friends or family or flushed if they are an old prescription).
Safety plans should ideally include all of the following components:
- Warning signs that the person may have experienced in the past that suicidal thoughts are starting to develop;
- Strengths and coping strategies that the person can use to stay safe;
- Who the person can reach out to for support/help;
- Steps that the person can take to make the environment around them safe, including reducing access to lethal means;
- Reasons for living that the person has identified during the conversation;
- Contact information for the county crisis team in their area, as well as a reminder that they can reach out to the 988 Suicide and Crisis Lifeline 24/7 for help as needed.
If the individual consents to follow-up services, the counselor should include some limited detail about the individual’s planned action for the follow-up counselor to check on during the follow-up activity (ex. the individual said they would call a friend and talk to them about what’s going on, the individual said they would make an appointment with their therapist the next day, etc.)
Follow-up Services
Purpose: Follow-up services provide opportunity to check-in with an individual who contacted the 988 Suicide and Crisis Lifeline to see how they’re doing, provide additional resources or connections to services, and complete additional assessment of the individual’s current level of safety and risk for suicide.
Definitions:
Safety Support Call: Safety support calls can be offered to individuals who contacted the 988 Suicide and Crisis Lifeline within 24 hours of initial contact to check for current level of safety and provide additional support (and if necessary, additional resources and/or intervention). These calls are offered as a more immediate wellness check than a Follow-up and can be offered to be within hours of initial contact. Safety Support calls are offered at the discretion of the Supervisor and 988 Crisis Counselor as needed.
Follow-Up: Follow-ups provide opportunity to check-in with an individual who contacted the 988 Suicide and Crisis Lifeline to see how they’re doing, provide additional resources or connections to services, and complete additional assessment of the individual’s current level of safety and risk for suicide.
Follow-up or Safety Support Contact Eligibility
A Follow-up contact should be offered to every individual who reaches out to Mental Health Minnesota’s 988 Lifeline Center and confirms current suicidal or homicidal ideation (at the time of the initial conversation or within the past 24 hours). Those deemed to be at moderate to high risk for suicide or homicidal ideation should be strongly encouraged to accept a follow-up call.
Scheduling a Follow-up or Safety Support Contact
During an initial 988 interaction, crisis counselors should ask if the contact is interested in, and consents to, a follow-up contact.
If an individual agrees to a safety support or follow-up call or text, it should be documented in that interaction record in iCarol and scheduled in the Unified Platform (Vibrant).
Safety support contacts should be scheduled within 24 hours of the initial interaction (often within a few hours of the initial interaction).
Follow-up contacts should be scheduled for 24-72 hours after the initial interaction. The crisis counselor and the individual should determine a specific window of time for follow-up to occur (ex. The following day between 2PM and 3PM).
The follow-up can be offered either as an SMS text or a phone call. Though Mental Health Minnesota only receives 988 texts and chats, the individual’s preference should dictate the modality.
The crisis counselor must schedule the follow-up or safety support contact in Vibrant. This will include contact information, the scheduled time and date, and a short note about the purpose/goal of the follow-up call (ex. checking on the individual’s current safety, checking to see whether the resources they were provided worked out, etc).
In addition to scheduling the contact in the Vibrant platform, crisis counselors must also include the time and date of the follow-up in the description/notes as a redundancy to ensure the follow-up is conducted at the appropriate time.
Making Contact
Safety support and follow-up contacts that have been scheduled are completed by the Follow-Up Counselor on duty when the follow-up activity is due, regardless of which counselor scheduled the follow-up activity. If there is no Follow-Up Counselor available, the supervisor on duty will conduct the contact or the supervisor on duty may assign it to a crisis counselor if it is a text follow-up.
Follow-ups are conducted by either phone or text. Text follow-ups are conducted through the Unified Platform (Vibrant). Phone call follow-ups are conducted through Mental Health Minnesota’s authorized phone system.
Individuals who have consented to a follow-up should receive a minimum of 2 follow-up contacts unless the contact does not consent to a second follow-up. Some individuals refuse further contact once their crisis has been addressed, so care should be taken to always request consent for further contact.
Unsuccessful Outreach Attempts
If the individual is not reached at the scheduled time, a minimum of three (3) total attempts should be made to make contact with the individual using the following guidelines:
- At least one of the three attempts should be made on a different day.
- For phone calls, this can include an initial call attempt. If no response, a second attempt approximately fifteen minutes later. If still no response, a third call should be made the following day at the originally scheduled time.
- For SMS text, an initial text follow-up should be conducted at the scheduled time. If there is no response within fifteen minutes, a second text attempt should be made. If there is still no response, the third attempt should be conducted the following day around the same time as the originally scheduled text.
- Sample text language for an unsuccessful second attempt could be: “Since we haven’t had a response yet, it seems this may not be a good time. I’m going to disconnect the chat from my end. We will try one more time tomorrow around the same time. Please know you can reach back out to 988, 24/7, if you ever need to.”
If an individual does not answer follow-up calls during the scheduled time and was deemed to be at high risk for suicide during the initial chat/text interaction, the counselor completing the follow-up activity should consult with the supervisor on duty to discuss any additional steps that may need to be taken, including a request for a safety/wellness check through law enforcement.
Best Practices of a Safety Support or Follow up Contact
During a successful follow-up contact, the following items need to be addressed:
- Assess the individual’s current well-being and safety. This includes asking the two required safety questions:
- “Have you had any thoughts of suicide in the past few days, including today?”
- “Have you taken any action to harm yourself today?”
- Collaboratively review and update Safety Plan as needed;
- Coordinate care with other providers if applicable; and
- Increase connection to needed services or offer additional resources if the contact consents.
Documentation
Counselors must document all follow-up contacts within the record in iCarol, including any action taken or hand-offs provided, additional resources provided, and level of current risk (determined by utilizing the safety assessment tool).
Counselors must also document all follow-up contacts within the Unified Platform (Vibrant).
Training
Follow-Ups Counselors will follow 988 Crisis Counselor training with additional training in peer support. Additional follow-up procedure documents and other resources are available before, during and after interacting with a contact.
Third Party Callers
Purpose: When it is determined that an individual is concerned about someone who may be suicidal, the counselor will actively engage the Third Party in a conversation to help determine the lethality of suicide, make a safety plan, and provide information and referrals, listening and support.
Evaluation of Risk
- The counselor will use a Suicide Risk Assessment to determine the lethality and imminence of suicidal death based on the information obtained from the Third Party.
- If the counselor determines that the threat of suicidal death is imminent, they will do what they can to connect the Third Party to law enforcement so the person with thoughts of suicide can receive a welfare check.
- If the counselor determines that the threat of suicidal death is not imminent, they can offer the option of a Third Party call, where the counselor calls the person with thoughts of suicide.
Third Party Calls
- If the Third Party chooses the Third Party Suicide Call option, the counselor will obtain the name, phone number, and location (including address, if available) of the person with thoughts of suicide, along with the name and phone number of the Third Party (a Third Party call will not be made if the original caller does not provide their name and phone number).
- The counselor will inform the Third Party that Mental Health Minnesota will not be able to release any information to them about the outcome of the third party call, and will tell the Third Party that they will call them back only if they are “not able to assess the risk” of the person with thoughts of suicide.
- The counselor will end the call with the original contact and attempt to reach the person who is potentially at risk of suicide but will not tell the person with thoughts of suicide the identity of the original caller.
- Third party calls are ended if the person potentially at risk of suicide doesn’t answer the phone on the second try, or when that individual collaborates with a safety plan and agrees to obtain help.
- If the counselor cannot reach the person potentially at risk of suicide after calling the number twice within one minute, they will call the original contact back, tell them that they were unable to assess the situation, and suggest either rescue procedures, calling/visiting the suicidal person, offering resources, or other appropriate suicide interventions.
Familiar Contacts
Purpose: The purpose of this policy is to provide guidance for supporting individuals familiar to the 988 Lifeline.
Definition: Familiar Contacts are individuals who have contacted 988 repeatedly and are identifiable by their phone number, name, IP address, the content of their conversation or other identifiable information.
Identification of Contact and Intervention
Counselors must follow all 988 Policies for Suicide Safety Assessment, Safety Planning and Intervention for every contact, including familiar contacts.
Once a familiar contact is identified, Counselors should notify their supervisor that they are in contact with someone familiar to the Lifeline. The Supervisor can confirm that the contact is familiar. The Supervisor can also confirm whether any particular limits have been placed on a contact due to the high volume of contacts or another reason. If no limits have been established but the Supervisor determines that some should be established, they should coordinate with the 988 Lifeline Manager to establish limits supportive to both the familiar contact and Mental Health Minnesota’s 988 commitment to service.
Once safety is assessed, supporting familiar contacts should be focused on assisting and advocating for their health, encouraging engagement with treatment providers, and adapting a Safety Plan or a Crisis response plan to promote agency.
Setting Limits
Mental Health Minnesota will not queue, block or ban any individual from contacting the 988 Lifeline.
The 988 Lifeline Manager may elect to establish specific limits with familiar individuals, particularly the length of text/chat. These limits are established on case-by-case assessments of familiar contacts. Limitations only take effect after a Sucide Safety Assessment is conducted and safety is assessed.
Requests for Specific Crisis Counselors
No contact may be transferred to a specific counselor, regardless if requested by the contact.
Communicating Notice of Familiarity and Limits
Crisis counselors may acknowledge they are familiar with the individual once familiarity has been confirmed with the Supervisor. Supervisors may opt to allow counselors to notify contacts of any limits placed upon their chats or text. Sample language may include: “In order to provide the best service, our conversations will be limited to 45 minutes.”
Ending Contact
Once it is determined that no further assistance is required and a limitation has been reached, explain you will end the contact and instruct the individual to reach back out if something changes and further help is needed. Sample language may include:
- “Since we reviewed all the options the Lifeline can offer and you are not in need of emergency assistance right now, I will be ending this conversation. Remember you can contact us again if your situation becomes more difficult and you need further help.”
Abusive Contacts
Purpose: To provide guidance on how to approach the management of abusive contacts while promoting the safety and well-being of both crisis counselors and individuals contacting the 988 Lifeline.
Definition: An abusive contact is someone who is utilizing Lifeline services in a way it is not intended, usually for the purpose of causing emotional distress or humiliation to the crisis counselor, interfering with service delivery for the center as a whole, or for personal gratification beyond emotional support.
Expectations for Responding to Abusive Contacts
Any contact reaching out to the 988 Lifeline must initially be assessed for safety and suicidal ideation, even if they’ve been previously identified as an abusive contact.
Safety for Staff and Crisis Counselors
The safety of staff and crisis counselors is critically important to promote a healthy and supportive work environment. If a contact becomes abusive, the Crisis Counselor must inform the supervisor and the supervisor must take all necessary actions to support the crisis counselor.
Procedure for Management of Abusive Contacts
Abusive, harassing, or sexually motivated contacts to the Lifeline can be very challenging, both clinically and operationally. Abusive visitors on chat will sometimes use language or describe content that is offensive to Counselors and elicits strong emotional reactions. It is important that Counselors feel safe and supported throughout any interaction with a contact. It is also important that Counselors are able to be clear with Contacts when their behavior is inappropriate and to know how to terminate the conversation if it does not improve.
It is important that Crisis Counselors try to assess the intention of a visitor’s comments before making the assumption that the visitor is being abusive. Some visitors, particularly youth, use swear words frequently without the intention of offending anyone. Some visitors may also describe graphic sexual content without the intention being harassing, such as describing an incident of sexual abuse.
Generally, a Contact’s behavior can be considered abusive if:
- The words or content are directed toward the Crisis Counselor;
- The behavior has not stopped after the Crisis Counselor has asked the Contact to cease the behavior; or
- In coordination with the Supervisor or Management staff, it is determined that the contact is being abusive.
Addressing the Abusive Behavior
One direct method for addressing abusive behavior is to re-state the purpose of the Lifeline and clearly define the abusive behavior. For example:
- “The Lifeline is for people who are feeling suicidal or in crisis and needing support. If you can stop (fill in behavior), I will be happy to keep talking. Otherwise, I will need to end the conversation.”
Terminating the conversation
The conversation can be terminated if:
- The Supervisor determines that the contact is abusive and is causing harm to the Crisis Counselor or Center;
- A threat, or continued abusive language, is directed at the Crisis Counselor; or
- An abusive visitor does not stop their behavior after a warning. A sample termination message could be:
- “I am going to end this conversation now because you are continuing to (specify behavior), goodbye.”
Tracking Abusive Contacts
Supervisors should inform their Manager of an abusive contact, including a brief description and/or other profile information so that they may be identified upon the next contact. This information shall not violate any HIPAA and Cybersecurity best practices and is to remain internal to the organization.
Concurrency: Two text/chat conversations on the 988 Lifeline Simultaneously
Definition: Concurrency is defined as when an experienced 988 Lifeline crisis counselor is conversing with two individuals on the 988 Lifeline simultaneously via text or chat.
Purpose: When specific conditions are met, experienced crisis counselors are expected to take two conversations at a time during their shift when possible. This allows the 988 Lifeline to better serve community needs during high volume times.
Philosophy: It is important to maintain a high quality of care for every individual seeking support from the 988 Lifeline. Taking a second text or chat conversation is an important step to broadening the reach of the 988 Lifeline, but it is critical that second conversations are accepted once specific conditions are met to ensure that high quality of care remains intact.
Conditions when a crisis counselor should begin a second (concurrent) 988 conversation:
- The crisis counselor is experienced and has at least 160 hours of experience.
- When the first chat is low-risk (after establishing safety) or is a Familiar Contact and low risk.
- When there is an appropriate amount of time in a crisis counselor’s shift.
Conditions when a crisis counselor should not take a second (concurrent) 988 conversation:
- High-risk conversations
- If the current help-seeker is at high risk, do not take a concurrent chat/text until they are deescalated and/or safe.
- Rapid-responding help-seeker
- If the current help-seeker responds very rapidly, it may not be suitable to take a concurrent conversation.
- Supervisor/Manager direction or at request of crisis counselor
- If the supervisor or manager determines that it is temporarily not suitable.
- If a crisis counselor believes they are temporarily unable to take concurrent conversations for another reason, they should speak with the supervisor.
Concurrency best practices:
- Process for ending concurrent chats/texts before taking another:
- Generally, once a crisis counselor takes a concurrent chat/text, both conversations should be fully concluded and documented before taking a new chat/text.
- Documentation:
- Crisis counselors have discretion on when to document each interaction. Always maintain high quality of service and attention to all active conversations.
- Debrief:
- Debrief as needed after both conversations have wrapped up. This can be independent debriefing or can include a supervisor.
- When interventions or rescues are needed:
- If one of the two interactions requires intervention, continue both conversations, inform the Supervisor, and be mindful of response times to the emergency.
- If high quality of service cannot be maintained for both conversations, request with the Supervisor that the non-emergency conversation be transferred to another counselor if possible.
Supervision of concurrent conversations:
Supervisors are expected to encourage concurrent conversations for experienced Crisis Counselors during their shifts following the guidelines listed above. Supervisors monitor chat traffic and overall shift performance and also have the authority to temporarily limit crisis counselors to one interaction at a time if deemed necessary. Generally, below is guidance for supervising concurrent conversations:
- Monitor chats as usual.
- Stay attentive for the potential to have to take over a chat or transfer a chat.
- Override concurrency if needed. Below are examples or situations where this might be necessary:
- If the center, supervisor or crisis counselor is over capacity to maintain quality of service.
- For example: If a Supervisor is required to conduct follow-ups, and has 5 staff all taking 2 chats (10 chats to monitor concurrently and conducting follow-ups) that may be well beyond capacity for the Center and Supervisor. The Supervisor can inform crisis counselors to take only 1 interaction at a time after their concurrent interactions.
- Supervisors can limit a counselor to 1 chat at a time if they determine it necessary.
- Technical issues – if there is a technical limitation restricting the monitoring or functionality of supervising.
- If the center, supervisor or crisis counselor is over capacity to maintain quality of service.
No Limitations of Services
Purpose: Mental Health Minnesota ensures that the 988 Lifeline service is open and accessible to all users.
Mental Health Minnesota does not ban, block or refuse to answer any 988 Lifeline chatters or texters.
No time limits may be placed on texters or chatters unless clinically appropriate for individual circumstances outlined in the “Familiar Contacts” and “Abusive Contacts” policy section of this document.
988 Warm Transfer
Purpose: To define warm transfers and provide guidance on ensuring counselors are appropriately meeting the needs of individuals in crisis when conducting warm transfers.
Definitions:
Warm Transfer: A warm transfer is a phone call-based transfer where a staff member is in contact with an individual in crisis and connects them to a resource inside or outside of the organization. It is a warm transfer as the staff member connects with the receiving organization, explains the situation and ensures that the individual in crisis establishes successful contact.
Procedure
Warm transfers are conducted via phone. Through the suicide and safety planning process a crisis counselor, follow-up counselor and/or supervisor will become aware of the potential need and benefits of a warm transfer. Some possible conditions where a warm transfer might be considered are:
- Connecting a contact with a mobile crisis team for further evaluation and possible in-person response;
- Connecting a contact to resources within the local area if they wish to have phone contact with someone;
- Connecting a contact to a center that is specifically trained to speak with specific populations (such as a Veteran’s crisis line) if they wish to have phone contact with someone;
- Connecting a Spanish-speaking contact in crisis to the Spanish Subnetwork if they wish to have phone contact with someone; or
- Connecting a contact with the LGBTQ+ Youth subnetwork (young people who identify as LGBTQ+ may wish to access specialized LGBTQ+ affirming crisis counseling but did not press “3”) and who wish to have phone contact with someone.
If those conditions, or other conditions determined necessary by the supervisor on duty, warrant a warm transfer, the counselor will request a phone number where the individual can be reached. The counselor will explain to the individual that the supervisor will call them in order to establish a phone connection. The supervisor will then call the individual via Mental Health Minnesota’s authorized phone system. The crisis counselor will keep the chat/text open if the individual is able to (if the individual is using their smartphone, they may not be able to keep a chat or text conversation open when receiving a call). The supervisor will communicate with the individual, locate the relevant resource and then conduct a warm transfer.
Warm Transfer Protocol
The supervisor must ensure that the individual consents to a warm transfer, explains what to expect during the transfer, speaks with the receiving organization or resource and explains the situation, stays on the line to confirm that the individual has established successful contact.
The procedures for a warm transfer through Mental Health Minnesota’s phone system are further detailed in training, materials and in-person shadowing and trainings.
Referrals and Resources
Purpose: Providing referrals and resources to external organizations and community-based support networks are profoundly valuable and fill an important role in the continuum of care that supports individuals seeking crisis services. It is important for staff to be aware of procedures regarding offering referrals and resources and the importance of providing individuals in crisis with options and the ability to choose the type of support they feel works best for them when different modalities and resources for support exist in the individual’s area.
Providing Referrals and Resources
988 Counselors, supervisors and follow-up counselors should seek to offer additional support to contacts by offering relevant resources and providing referrals to a variety of social service organizations, governmental and crisis programs, agencies and organizations.
After assessing safety, referrals and resources can be offered depending on the individual’s needs and preferences. If the counselor determines that an individual may benefit from a resource or referral, they may ask the individual if they are interested in hearing about them. Referrals and resources should only be given if the individual consents.
If the individual consents and is interested in a resource or a referral, the counselor should provide the information and connect them as best fit to the support that they need.
Referral and Resources Database
Mental Health Minnesota maintains an updated list of resources for Minnesota. This resource list is available to counselors and supervisors during 988 Lifeline conversations via the Google Drive resource folder.
Primary approved resources and referral networks are bookmarked for each counselor and supervisor. These can include the 211 database, a list of mobile crisis contacts, FastTrackerMN, PSAP locators and others.
Violence and Threat Assessment
Purpose: There may be an occasion when an individual contacts the 988 Lifeline and is experiencing violent or homicidal ideation. It is important for crisis counselors to be equipped to identify threats of violence, assess potential risk and assist in the development of a safety plan when supporting individuals who are experiencing violent and/or homicidal ideation.
Procedure
If an individual contacts the 988 Lifeline and is experiencing violent or homicidal ideation, the procedure is similar to that of an individual experiencing suicidal ideation. The Suicide Safety Assessment, Safety Planning and Intervention section outlines the procedure to assist and assess an individual’s situation. If violent threats of homicidal ideation is present during the interaction, follow the procedure in the Suicide Safety Assessment, Safety Planning and Intervention section.
Connect with the individual, assess their current safety and identify Desire, Capability, Intent and Buffers for violence and homicidal ideation just as suicidal ideation.
Potential Risk Factors
While conducting the assessment, potential risk factors to be aware of include:
- Direct or indirect threats of violence
- History of violence
- Recent stressors (job loss, divorce, legal troubles, etc.)
- Substance use
- Agitation or irritability
- Difficulty taking responsibility for one’s actions or a fixation upon blaming others
- Suicidality: Suicidal ideation is seen in many perpetrators of violence and individuals with homicidal ideation are statistically more likely to harm themselves than to harm others. (Note: Iindividuals may present with suicidal and homicidal thoughts simultaneously and may portray their thoughts of homicide as acts of mercy toward their indended targets.)
- Symptomatic psychiatric illness, especially psychosis. (Note: Individuals with mental health diagnoses are far more likely to experience violence than to be perpetrators of violence.)
Artificial Intelligence (AI) Usage
Purpose: To offer clear policy regarding the use of Artificial Intelligence tools and software related to 988 services and to clarify why their use is prohibited.
Definitions:
Artificial Intelligence (AI) generally refers to machine-based systems and software that can make predictions, recommendations, or decisions for a user.
Generative AI tools, generally, are machine learning tools that analyze massive amounts of data and information to learn patterns in order to create novel text, audio, images, video, etc. Generative AI tools require inputs from a user often referred to as ‘prompts’ or questions, which are then used to generate creative content for the user.
Privacy, Confidentiality and Security:
Mental Health Minnesota protects and respects the privacy of every individual that reaches out to 988. Help-seekers are expressing their most vulnerable moments to crisis counselors. These moments are confidential and private.
Any use or input into an AI software related to a 988 interaction constitutes a breach in confidentiality and privacy and is strictly prohibited. AI tools use machine learning that document all inputs and record them on their servers. Inputting any question, text or prompt related to a help-seeker into an AI software would be no different than telling a stranger, a corporation or other entity private information about a help-seeker, whether that information is direct or inferred.
AI Usage is Prohibited:
If an employee at Mental Health Minnesota is found to be using an AI software to input help-seeker’s text or situation and/or generate text responses for 988 text or chat services, it may be considered cause for immediate termination.
Examples of AI tools and software:
Examples of AI software with generative content include: ChatGPT, Jasper AI, CopyAI, Claude, Grammarly, Microsoft Copilot and virtual assistants such as Alexa, Siri and Google Assistant. These are only examples, there is an ever growing number of these tools.
Support for Crisis Counselors:
If counselors want or need assistance in responding to an interaction with a help seeker, they should reach out to supervisors, managers or fellow counselors. Mental Health Minnesota managers and supervisors are there to support crisis counselors and staff with best practices and supportive language as needed.
988 Lifeline Supervision
Purpose: Supervision is provided of 988 Lifeline Counselors to ensure that Mental Health Minnesota provides high-quality, consistent service to those interacting with the 988 Suicide and Crisis Lifeline, as well as to ensure that Lifeline Counselors have the support they need during text/chat interactions.
Supervisor Responsibilities
Supervisor responsibilities include but are not limited to:
- Providing guidance, supervision, support and oversight to 988 Lifeline Counselors during text/chat interactions;
- Ensuring that staff and volunteers follow established policies, procedures and protocols
- Supporting staff and volunteers as needed to process/discuss calls that are challenging or triggering
- Assisting staff and volunteers in implementing warm hand-offs to county crisis services
- Making determinations regarding use of emergency services based on organizational policy, and facilitate calls to 911 dispatch as needed
- Ensuring that data forms are completed, and reporting concerns or issues to program managers as needed (including a report anytime that an active rescue is initiated, whether voluntary or involuntary)
- Participating in the training and onboarding process for new counselors and/or supervisors as requested by the 988 Lifeline Manager;
- Attending staff meetings and meeting as needed with 988 Lifeline Manager and Peer Support Programs Manager
- Addressing/troubleshooting concerns and technology issues that arise during assigned shifts
- Assisting with responding to calls, texts and chats as appropriate and needed to ensure availability of services
Record Keeping
Purpose: Confidential records of all text and chat interactions are maintained for data tracking, reporting and ongoing quality assurance.
Data Collection Tool
- Records of interactions through the 988 Suicide and Crisis Lifeline are held in a confidential, encrypted database.
- Mental Health Minnesota utilizes iCarol as its data collection tool. Confidential data about individuals using the 988 Lifeline and the text/chat interaction must not be retained in any other format.
Data Collection
- Data must be collected for each text/chat interaction, completing as many of the form fields as possible.
- Data collected includes:
- Individual demographic data (i.e. county, and other demographic information as available)
- Assessment of individual safety/risk of suicide and recording of level of risk
- Disposition of the interaction/actions taken by the counselor
- Resources provided to the individual
- Whether a safety plan was established with the individual
- Whether a hand-off to mobile crisis services or an active rescue took place
- Follow-up needed, as well as contact information for the provision of follow-up services
Use of Data Records
- Reporting: Data records for 988 are utilized for reporting as required by the Minnesota Department of Health and/or Vibrant Emotional Health. Data used for reporting purposes is aggregated, not provided on individual interactions.
- Quality Assurance: Data records for 988 are also used by program management to ensure high quality service is provided, that interventions and resources are being used appropriately, and to review situations in which an involuntary active rescue was initiated. Data records for this purpose may be aggregated or reviewed on an individual basis.
- External Requests for Records: It is our policy not to release records of any 988 interactions outside of the agency without a court order, except in imminent risk situations. Any requests for 988 transcripts or records must be coordinated directly through Vibrant Emotional Health.
- Record Retention: Records will be maintained for a minimum of three (3) years.
Program Evaluation and Quality Assurance
Purpose: To ensure high quality 988 Lifeline Center response, Mental Health Minnesota sets program goals and objectives, works to track and measure outcomes and outputs, and utilize data and the experience of both employees and individuals served for program quality assurance and improvement.
Program Evaluation
The 988 Lifeline program’s effectiveness and quality are measured through data collection, as well as through review of text/chat transcripts and the disposition of interactions/actions taken by 988 Lifeline counselors.
Data Collection
The data collection tool and process are included in the Mental Health Minnesota 988 Lifeline Center’s Policies and Procedures: Record Keeping.
Program Objectives and Evaluation
Mental Health Minnesota sets program objectives and goals for the 988 Lifeline Center to ensure high quality service and works toward continuous improvement. Objectives and projected outcomes are reviewed annually. Program evaluation occurs on a regular basis (depending on the measure).
- Program Objective #1: Respond to 100% of the text and chats that are routed to Mental Health Minnesota’s 988 Lifeline Center.
- Evaluation strategies: Review of data from Vibrant Emotional Health on response rate; evaluation of overall in-state response rate to assess additional staffing needs at various times of the day
- Evaluation strategies: Review of data from Vibrant Emotional Health on response rate; evaluation of overall in-state response rate to assess additional staffing needs at various times of the day
- Program Objective #2: Provide follow-up texts/chats to individuals who connect to Mental Health Minnesota’s 988 Lifeline center to ensure continuity of care with each individual
- Evaluation strategies: Tracking of percent of follow-up activity based on total number of interaction and relationship to level of risk for suicide during assessment
- Evaluation strategies: Tracking of percent of follow-up activity based on total number of interaction and relationship to level of risk for suicide during assessment
- Program Objective #3: Ensure that individuals served by Mental Health Minnesota’s 988 Lifeline Center are evaluated appropriately for safety/risk of suicide, and that the level of intervention provided is the least intensive intervention possible
- Evaluation strategies: Review aggregate and individual records to assess whether the level of intervention matched the need based on the assessment; evaluate data by counselor to assess individual performance and decision making; review transcripts from chats/texts for new counselors; review transcripts/comments from Vibrant Emotional Health; review all interactions that resulted in an active rescue (after each situation)
- Evaluation strategies: Review aggregate and individual records to assess whether the level of intervention matched the need based on the assessment; evaluate data by counselor to assess individual performance and decision making; review transcripts from chats/texts for new counselors; review transcripts/comments from Vibrant Emotional Health; review all interactions that resulted in an active rescue (after each situation)
- Program Objective #4: Work toward continuous improvement of 988 Lifeline response through evaluation of data and the outcome of interactions (individual and aggregate), user experience and employee feedback.
- Evaluation strategies: Evaluate data collected on individual interactions to better understand service use and identify training needs; identify additional employee training needs through employee reviews/feedback; identify additional training and resource needs based on demographic data
Quality Assurance
Program evaluation measures are utilized by program coordinators and management to ensure high quality service is provided, that interventions and resources are being used appropriately, and to review situations in which an involuntary active rescue was initiated. With an aim toward continuous improvement, data records may be aggregated or reviewed on an individual basis, and employee feedback will also be considered for the following purposes:
- Assurance that high-quality text and chat services are being provided, as well as that risk of suicide is being evaluated and documented properly and that the appropriate level of intervention is provided
- Consideration of new or additional training and/or resources that may aid 988 Lifeline counselors in their work
- Evaluation of 988 Lifeline counselors and supervisors on an individual basis for the purposes of coaching and learning
Quality Assurance – Contact Monitoring
- To adhere to the Lifeline Administrator’s quality standards, Mental Health Minnesota will aim to exceed the quality standard of 90% of all crisis counselors taking 988 interactions achieving a QI score of 70% or higher (monthly) and a 70% or higher overall center score (quarterly). The QI score will be defined by the 988 Lifeline Administrator.
- Mental Health Minnesota will monitor, at minimum, 1% of 988 Lifeline contacts per month, utilizing the 988 Lifeline Quality Improvement (QI) Monitoring Form provided by the 988 Lifeline Administrator.
- Mental Health Minnesota will monitor each counselor at least once per quarter
- Mental Health Minnesota will monitor new counselors at least three times within their first three months.
- Mental Health Minnesota will respond to requests from the 988 Lifeline Administrator to review specific interactions resulting from the Administrator’s own contact monitoring, grievance process and/or sentinel event or loss notification.
- Quality Assurance supervisory staff shall undergo training consistent with the above objectives.
Quality Assurance – Contact Monitoring Training
Training is a necessary component for promoting consistency and confidence in contact monitoring across supervisory staff.
Mental Health Minnesota will provide the Compliance and Training Manager, Program Managers and any other designated QI Specialist with training on how to monitor contacts and review interactions in accordance with this policy. Training material will include:
- Training on the technology used to conduct reviews and monitoring.
- The 988 Lifeline Administrator’s clinical standards that should be reviewed during monitoring.
- Scoring of interactions including the tools utilized and thresholds.
- How feedback and coaching will be provided to crisis counselors following the monitoring of an interaction.
Complaints and Grievances
Purpose: Mental Health Minnesota strives to ensure that all contacts are treated in a professional and respectful manner. The purpose of the Complaints and Grievances policy to outline guidance if a contact submits a complaint or grievance with Mental Health Minnesota’s services.
Complaints and Grievances Procedure
988 Counselors should direct any complaint to the Supervisor on-duty. The Supervisor should:
- Gather information about the complaint, including phone number or IP Address the caller used at the time of contact, the date and time of the contact, and the nature of, or detail of, the complaint; and
- Encourage the 988 counselor to direct the chatter/texter to submit a written complaint to the 988 Lifeline Manager if they wish to do so.
Once the complaint or grievance information is gathered, the information should be passed onto the 988 Lifeline Manager.
The 988 Lifeline Manager should then investigate and review the conversation for compliance with 988 Lifeline clinical standards and operating requirements. If the investigation suggests a corrective action or training is required to address the issue, those actions should be taken with the 988 counselor or individual named in the complaint.
Mental Health Minnesota will provide a written record describing the nature of the complaint and its resolution, and forward the details within 24 hours of completing the investigation, to the 988 Lifeline Administrator via encrypted email to [email protected].
Mental Health Minnesota will also notify the Minnesota Department of Health within 48 hours of becoming aware of the complaint.
Complaint or Grievance from Another Crisis Center
If a contact has a complaint or grievance with services provided by another crisis center, the Supervisor can suggest that the 988 Counselor direct the individual to submit their complaint or grievance to the 988 Lifeline Contact Us Page: https://988lifeline.org/contact-the-lifeline/
If the individual is not capable or willing to do that, the supervisor can gather information about the complaint, including phone number or IP Address the contact used at the time of contact, the date and time of the contact, and the nature of, or detail of, the complaint. This should be elevated to the Lifeline Manager, who can then reach out to the 988 Lifeline Administrator, ideally within 24 hours of receipt of complaint.
Written Complaint or Grievance Forwarded from the 988 Lifeline Administrator
If a complaint or grievance is received via Vibrant that pertains to services provided by Mental Health Minnesota, the following actions should be taken.
- Upon receipt of the complaint, Mental Health Minnesota shall submit a response in the provided format within one week of its receipt (unless otherwise noted). This response should include a review of the complaint and any resulting actions taken by Mental Health Minnesota.
- If more information is requested by the 988 Lifeline Administrator with respect to the status of a complaint or investigation, Mental Health Minnesota will provide it within a reasonable timeframe.
Written Records of Complaints
Mental Health Minnesota shall maintain a written record of any complaints or grievances, as well as document any resolution or steps taken to address them.
Sentinel Events
Purpose: To provide guidelines and procedures for identifying, reporting, reviewing, and preventing sentinel events at Mental Health Minnesota.
Definition: Broadly, a Sentinel Event is an unexpected occurrence involving death, serious physical injury, or a “near miss.” In the 988 Lifeline context, Sentinel Events include, but are not limited to, 988 Lifeline interactions or 988 delay in services followed by serious injury or death.
Mental Health Minnesota Reporting of Sentinel Events
If Mental Health Minnesota becomes aware of a Sentinel Event, the organization has the responsibility to report the event to the Lifeline Administrator promptly and accurately to [email protected] (using encryption to protect Personal Identifiable Information).
Mental Health Minnesota will disclose a Sentinel Event to the 988 Lifeline Center Network within 24 hours of discovery. The disclosure will include as much accurate information as possible about the Sentinel Event. This information must include:
- Contact information for the individual(s) involved;
- Any other relevant circumstances surrounding the incident;
- Any contributors to the incident as understood at this stage; and
- Any pre-identified steps being taken to prevent future occurrences.
Mental Health Minnesota will also notify the Minnesota Department of Health of critical incidents where a 988 help-seeker has died by suicide (Sentinel Event) within 48 hours of becoming aware of the event and within 7 days of the contact with Mental Health Minnesota’s 988 Lifeline Center.
If the 988 Lifeline Administrator becomes aware of a Sentinel Event occurring pertaining to Mental Health Minnesota, they will notify SAMHSA, the State (if applicable) and the Center Engagement Manager within 24-business hours. Then Minnesota Mental Health will be provided with the Sentinel Event Report form for completion.
The Sentinel Event Report form will be completed and returned to the 988 Lifeline Administrator for review within five (5) business days of its receipt. If certain events require an urgent or expedited response due to the nature of the concerns or ongoing concern for safety, it may be required to return the completed form within 24-48 hours.
The 988 Lifeline Administrator may follow up or request documentation and other materials after the Sentinel Event has been reviewed by the Administrator.
The review will be considered completed once all requested documents are received, reviewed and approved by the 988 Lifeline Administrator. Any feedback or recommendations will be provided to Mental Health Minnesota within five (5) business days of the completed review, as well as updates provided to SAMHSA and to the state when indicated.
Confidentiality will be maintained during the reporting process, with information shared only on a need-to-know basis and adhering to HIPAA regulations.
The 988 Lifeline Administrator will also connect Mental Health Minnesota to ongoing support where indicated (not limited to: the 988 Lifeline Wellness Team; Standards, Training, and Practices; etc.)
Review and Analysis by the 988 Lifeline Administrator
The 988 Lifeline Administrator will maintain open and transparent communication with Mental Health Minnesota as appropriate throughout the review process. Upon receipt of a Sentinel Event report, an immediate review will be initiated by the Administrator. The goal of the review is to identify contributing factors which may exist at all levels, to include individual and systems-level contributors.
The 988 Lifeline Administrator Sentinel Event reviews undergo a multidisciplinary approach and may include but aren’t limited to representatives from relevant departments within the Administrator. Mental Health Minnesota, and any other relevant parties, will provide all investigation documentation or records, as applicable by law and any other related policies.
Corrective Actions, Preventative Measures, and Crisis System Review
The 988 Lifeline Administrator recognizes that Sentinel Events can occur even when everything has been done according to 988 best practices. The Administrator may provide feedback to Mental Health Minnesota that could include a Performance Improvement Plan (PIP) to address identified areas for improvement with the intent of decreasing the likelihood of similar Sentinel Events in the future through expansions in policies, procedures, training and monitoring. Corrective actions aim to minimize harm to individuals contacting the 988 Lifeline for emotional distress or thoughts of suicide, improve systems and processes, and enhance public safety. A comprehensive record of the Sentinel Event, the review, corrective actions and preventive measures will be maintained by the Administrator and shared with Mental Health Minnesota and SAMHSA.
Code of Ethics
Purpose: The purpose of the code of ethics is to protect the rights of individuals provided services by Mental Health Minnesota’s 988 Lifeline Center, to ensure compliance with professional and community standards of conduct, and to provide guidelines for the resolution of ethical conflicts in suicide prevention and crisis intervention procedures.
Principles
Integrity
The crisis worker shall place the highest value on integrity. Whether as a counselor, supervisor, volunteer or manager, there should be no compromise with the best interests of the individuals served being the overriding consideration at all times.
Competence
Responsibility should only be undertaken or assigned for those activities for which the person has been trained and has demonstrated an adequate level of competence. If the needs of the person being helped are beyond the competence of the crisis worker, referral to someone with the needed skills should be accomplished as expeditiously as possible, assuring that possible feeling of rejection or abandonment are appropriately dealt with.
If lack of competence is observed in other persons or agencies, the observation should be made known to one’s supervisor or to the individual responsible for taking corrective action.
If physical or emotional concerns interfere with the crisis worker’s optimal functioning, appropriate steps should be taken to see that such problems do not compromise the quality of services offered. The interests of the person being helped are first dealt with, and measures to correct the crisis worker’s concerns instituted as well. Further crisis work should be deferred until such concerns no longer interfere with the person’s competence.
Moral Standards
The crisis worker should respect the social and moral attitudes of the community in which they work, assuring that the reputation of persons or agencies not be unnecessarily jeopardized.
Legal Standards
In the course of crisis work, illegal actions by the person in crisis should not be encouraged or facilitated. If the crisis worker recognizes a potential legal issue, of which the person is not aware, the crisis worker should inform the person of that issue. In no case should the crisis worker participate in an illegal act.
Representation
The crisis worker shall accurately represent their qualifications, affiliations and purposes when appropriate. The crisis worker should not provide information that would imply the presence of qualifications or affiliations, professional or otherwise, which are not accurate, or would lead others to assume qualities or characteristics that are not correct. If misrepresented by others, or if others make incorrect assumptions, the crisis worker should rectify such misconceptions.
The crisis worker should not use their affiliation with Mental Health Minnesota or the 988 Suicide and Crisis Lifeline for purposes which are not consonant with the stated purpose of that organization.
Public Statements
All public statements, whether direct or indirect, should be accurate and free of sensationalism, bias, distortion or misrepresentation of any kind. Special care in this regard is required in activities related to news articles aimed at stimulating public awareness and support of Mental Health Minnesota, and for solicitation of funds to continue the organization’s work.
When information is provided to the public about suicide prevention or crisis intervention techniques, it should be made clear that such techniques are to be used only by persons adequately trained in their use, when that is the case.
Confidentiality
Maintaining the confidentiality of information about individuals helped is a primary responsibility. Such information should not be communicated to others unless specific provisions for such release are met according to state statutes.
Confidential information may be revealed after careful consideration indicates the presence of clear and present danger to an individual or to society, and then only to those who must be informed in order to reduce that danger.
Information about persons being helped is discussed only with others concerned with the case.
Except for the situations noted above, information may be disclosed to another individual only when the individual being helped gives permission. The individual should specify what information may be given, and to whom. In circumstances judged by the crisis worker to constitute an emergency involving a threat to the life or safety of the person being helped, these restrictions may be suspended as necessary to provide the required assistance.
Written and oral reports should contain only information germane to the purpose of the report. Every effort should be made to protect the individual’s privacy.
In training and reporting, care should be taken that any material used that reflect actual interactions must be presented in such a way that the identity of the individual is not revealed.
The crisis worker should assure that appropriate provisions are made for the maintenance of confidentiality in the storage, retrieval, use, and ultimate disposition of records, including any written notes from the interaction.
Welfare of Individuals Receiving Crisis Services
If it becomes clear that the individual the crisis worker is responding to would best be served by referral to another crisis worker or another type of assistance, such referral should be accomplished without undue delay. Full consideration should be given to the possible adverse effects of referral, and the procedure carried out in such a manner that these potential adverse effects are minimized.
In the event of referral, the referring crisis worker should continue to render assistance as needed, until such time as the responsibility for helping the person is assumed fully, if that is appropriate, by the worker taking over the case.
Relationship with the Person Receiving Crisis Service
Crisis services should be provided only in the context of a professional type of program.
No illegal interaction should transpire in the course of providing crisis services.
The crisis worker should not provide services to their associates, friends or family members except in the most unusual circumstances, and then only with the concurrence of an experienced consultant.
Offering of Services
Provision of suicide prevention and crisis services should be carried out within strict limits of community standards, propriety and good taste.
Notices designed for public use, such as posters or brochures, may contain Mental Health Minnesota’s name, accreditation, the services offered, a description of those services, circumstances in which the services might appropriately be used, and how to obtain them. Reassurances, such as emphasizing 24-hour readiness to respond and desire to be of help, may be included in materials from Mental Health Minnesota.
No evaluative statements or assurance of quality or efficacy should be expressed or implied in any form.
Professional Relations
The integrity, traditions and potential helping role of all professions and disciplines should be acknowledged and respected, both in relations between disciplines and in communications with persons in crisis. No suggestion of precedence among disciplines should be expressed or implied, though special needs may call for unique skills in individual cases.
Crisis workers should not knowingly enter into a competitive role with other providers in the community. If the person being helped has a previously established relationship with another caregiver, the crisis worker should attempt to integrate the efforts being made. In no case should there be an effort to prevent the other caregiver from being informed of the crisis worker’s role. Mutual agreement of all concerned, as to the best way to assist the person in crisis, should be striven for.
Remuneration
No commission, rebate, or other consideration or inducement should be involved in a referral to or from a crisis worker for the provision of crisis services.
The crisis worker should not use their relationship with the individual being helped to promote their own benefit or that of any organization or of any other enterprise.
A crisis worker associated with another organization or institution should not accept a fee or other form of remuneration for providing services to an individual who is entitled to those services through the organization or institution.
A crisis worker should not accept a gift from a person being helped.
Ownership of Materials
All materials prepared by a crisis worker, in carrying out their regular duties at Mental Health Minnesota, shall be the property of that organization.
Materials prepared by a crisis worker at Mental Health Minnesota, other than those materials resulting from their regular duties, shall, if published, and the organization so desires, include a disclaimer of responsibility on the part of the organization for the content of the published materials.
Training for 988 Lifeline Counselors
All 988 Lifeline Counselors and Supervisors are required to complete 50+ hours of training prior to beginning active response to texts and chats as part of the 988 Suicide and Crisis Lifeline.
Training for the 988 Lifeline emphasizes a conversational approach to crisis/suicide assessment. It focuses on establishing and maintaining the help seeker’s sense of connection to the crisis counselor while assessing suicide and de-escalating the crisis. The training also is sensitive to populations disproportionately affected by suicide and cognizant of historically marginalized communities.
All new staff will be enrolled in required training and will receive login information for the Relias Online Learning Platform and the Lifeline Learning Center portal. Each training section must be completed before the next section can begin, and completion of all training components (including 8 live role-plays, 10 hours of live observation and meetings) must be documented in Relias. All staff are required to clock in and out for all training activities.
Additionally, ongoing annual training totalling 6 hours or more will be required. This will include cybersecurity and privacy awareness training, updated clinical guidance and/or 988 Lifeline webinars/self-paced training courses and/or wellness training.
Questions regarding training requirements and expectations can be directed to Mental Health Minnesota’s Compliance and Training Manager at [email protected].
Note: The sample training plan below is subject to change based upon new or updated training relevant to best practices for the 988 Lifeline Center.
| Section 1: Initial Orientation Activities (in office) | Hours |
| *In Office: General Orientation/Paperwork/Office Tour/Intro to BambooHR/Review of Employee Handbook/Finalize training schedule/Sign training agreement | 1 |
| *In Office: Initial Observation of 988 Lifeline Center Activities | 1 |
| Total Initial Orientation Activities | 2.0 |
| Section 2: Orientation online modules (begin training in Relias) | Hours |
| Mental Health Minnesota 101 | 0.5 |
| Mental Health Minnesota Employee Assistance Program Overview | 0.5 |
| Total Orientation online modules | 1.0 |
| Section 3: Fundamentals | Hours |
| About the Mental Health Crisis System (videos) | 0.25 |
| Maintaining Professional Boundaries | 0.5 |
| Privacy and Confidentiality for Non-HIPAA Covered Entities | 0.25 |
| An Overview of Trauma-Informed Care for Non-Clinical Staff | 1.0 |
| Understanding and Minimizing Cultural Bias for Paraprofessionals: | 1.0 |
| Serving LGBTQ Young People on 988 | 1.0 |
| Exploring the Need for Cultural Consideration in Youth Crisis Care | 1.0 |
| Using a Strengths-Based Approach with Children and Youth for Paraprofessionals | 0.75 |
| Non-Suicidal Self-Injurious Behavioral in Children and Adolescents | 1.0 |
| Cybersecurity & Phishing Training | 0.5 |
| Mental Health Minnesota – Wellness Training | 0.5 |
| Crisis Counseling with Rural Populations | 0.5 |
| Meet w/Compliance and Training Manager to discuss progress, questions | 0.5 |
| Total Fundamentals Training | 8.75 |
| Section 4: Crisis Counseling | Hours |
| Fundamentals of Crisis Counseling | 2.0 |
| Essential Skills in Crisis Counseling | 2.0 |
| Assessing Safety and Suicide Risk | 2.0 |
| Imminent Risk of Suicide | 2.0 |
| Crisis Conversations on Text and Chat | 2.0 |
| Cultural Responsiveness on Chat and Text | 1.0 |
| Follow-Up on the 988 Lifeline | 1.0 |
| Substance Use and People in Crisis | 1.0 |
| Individuals Familiar to the Lifeline | 1.5 |
| Lethal Means Counseling | 1.0 |
| Meet w/Compliance and Training Manager to discuss progress, questions | 0.50 |
| Total Crisis Counseling Training | 16.0 |
| Section 5: Practice/Simulation | Hours |
| Practice Activities: Cultivating Self-Awareness, Moving Forward After Challenging Interactions, The Language You Use, Understanding Expressions of Anger, Asking about Suicide | 1.5 |
| Simulation Exercise: Crisis Conversation Skill Builders | 2.0 |
| Simulation Exercise: 988 Direct | 0.75 |
| Simulation Exercise: 988 Third Party | 0.75 |
| Simulation Exercise: 988 Veteran | 0.75 |
| *Live meeting: Safety Planning | 0.5 |
| *Live meeting: Data Entry/Scheduling Follow-Ups | 0.5 |
| *Live meeting: Interventions and Warm Hand-offs | 0.5 |
| *Live meeting: Live Roleplays (8) with Training Manager. Network Resource Center overview. | 3.75 |
| *In Office: Observe multiple counselors as they respond to 988 Lifeline texts/chats | 9.0 |
| Total Practice/Simulation Training | 20.0 |
| Section 6: Policies and Procedures | Hours |
| Review 988 Lifeline policies and procedures/sign off on policies | 1.5 |
| Meet w/988 Lifeline Manager to discuss final questions or concerns | 1.0 |
| Total Policies and Procedures Training | 2.5 |
Appendix: Safety/Risk Assessment Tool
Full Safety Assessment for Suicide Risk/Concerns
Check the box under low, medium or high risk in each area (Desire, Buffers, Tabulate and utilize the score, along with clinical judgment (yours and your supervisor’s), to help with your assessment related to the individual’s safety and/or risk of suicide. Note that the areas that have an asterisk (*) are essential components of a full safety assessment, with the other items to be completed as needed/applicable. This tool is also in the iCarol system, to be completed as part of individual text/chat interaction records.
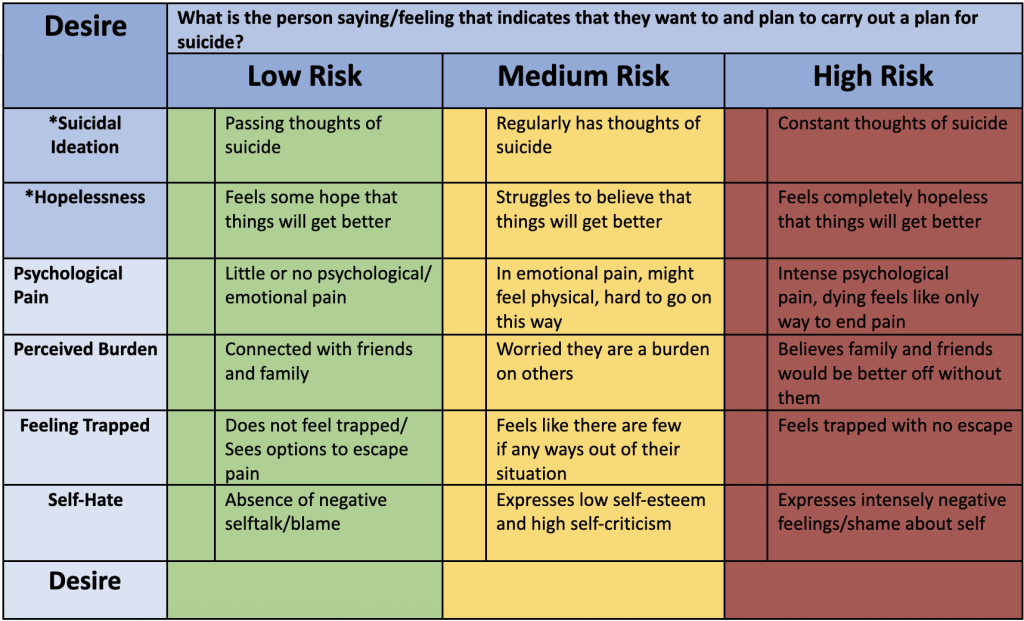
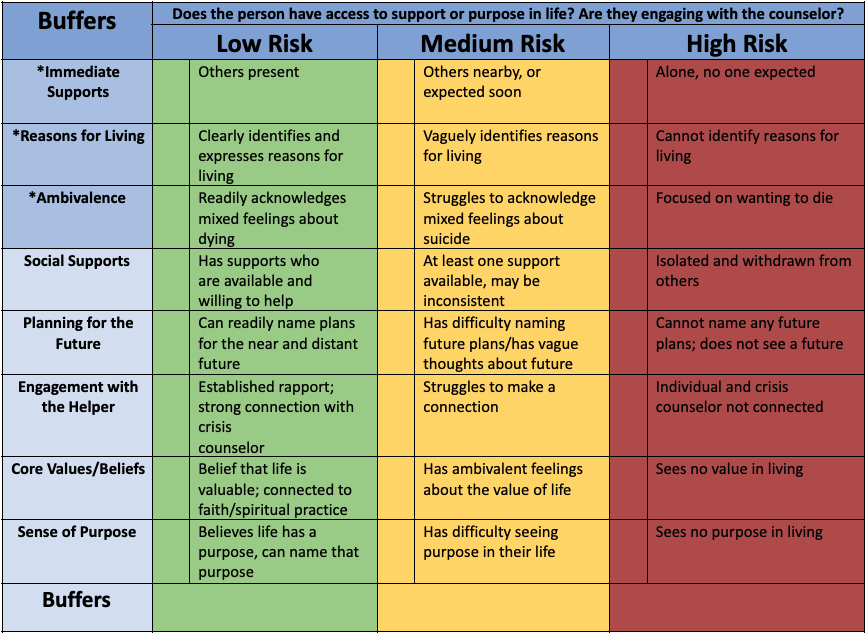

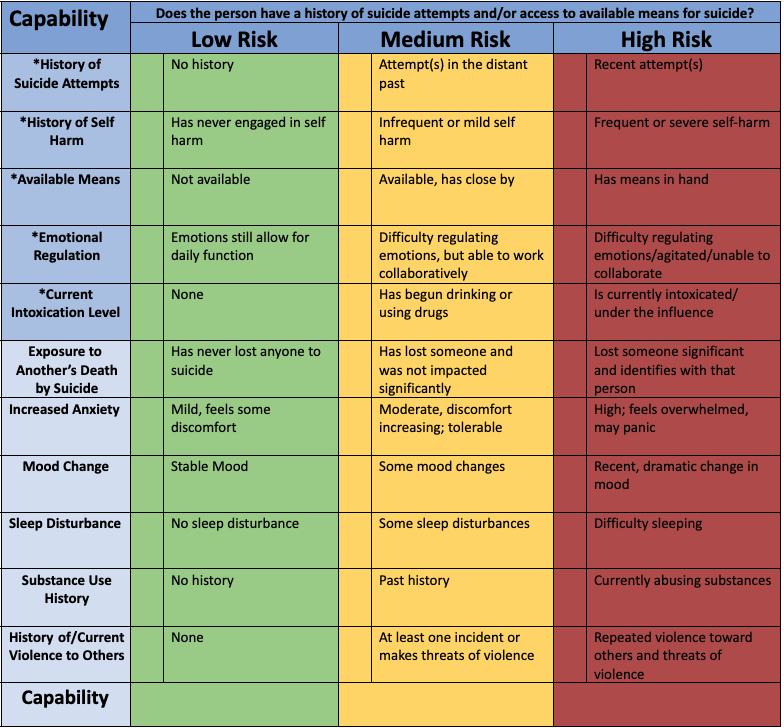
If the individual indicates previous suicide attempts, note method(s) used:
__________________________________________________________________________________________________________________________________________________________________________________________
Appendix: Safety Planning Tool